Cleaning and disinfection in health care settings during the COVID-19 outbreak

Related content
Cleaning and disinfection of the health care environment plays an important role in reducing indirect transmission of SARS-CoV-2 – the virus responsible for COVID-19.
SARS-CoV-2 can remain viable for between eight hours and several days, depending on the type of surface.1 Surfaces become contaminated when virus-containing droplets land on them, or when someone with contaminated hands touches these surfaces.
Decontamination of the health care environment is therefore vital. It includes cleaning, disinfection and the safe disposal of waste. In this article, we focus primarily on cleaning and disinfection; safe waste disposal will be discussed in more detail in a future issue of Community Eye Health Journal.
Cleaning is a process which removes contaminants, such as dust or microorganisms, and the body fluids (or organic matter) that shield them. Disinfection is the process by which any microorganisms that remain after cleaning are reduced to a level at which they are not harmful, which is only effective if the equipment or surface is thoroughly cleaned with a detergent solution beforehand.1
In the health care environment, we must clean and disinfect surfaces such as walls, floors, furniture, sinks and taps, stairway rails, touch screens, counter tops, door handles and light switches; and equipment such as torches, ophthalmoscopes, trial lenses, slit lamps, and wheelchairs, to name a few!
Standard cleaning and disinfection protocols continue to apply during the pandemic, but may have to take place more often. This article is based on guidance from the World Health Organization (bit.ly/COV19clean), national bodies and current research, but we also strongly recommend that you follow national guidelines.
Management of cleaning and disinfection
It is important that cleaning and disinfection practices are closely monitored, and that personnel responsible for cleaning have the correct PPE and are trained properly.
In the hospital setting, the infection control team is responsible for developing and approving cleaning and disinfection policies and strategy. Assigning cleaning duties, setting up cleaning schedules and checklists, and monitoring cleaning and disinfection practices is the responsibility of matrons, domestic supervisors and service managers.
Appropriate PPE must be worn during preparation of cleaning products and while cleaning: heavy duty gloves, face mask, eye protection (safety goggles or a face shield), a gown and closed work shoes. Note: heavy-duty gloves must be cleaned and disinfected before moving from one area to another, e.g., when moving from the outpatients waiting room to an examination room, and vice versa.
Everyone who is responsible for cleaning in the health care environment must be trained in:
• Safe disinfectant preparation
• Cleaning methods and equipment use
• Standard precautions
• Risk assessment and transmission-based precautions.
Preparation
Ideally, use fresh cloths and prepare fresh solutions of detergent and disinfectant for each cleaning shift. Rinse and dry mops and buckets between shifts. Detergents and disinfectant solutions applied from a bucket with a cloth or mop will become contaminated during cleaning and progressively less effective. Continued use of the same detergent or disinfectant solution may transfer microbes to each subsequent surface.
Always refer to the manufacturer’s instructions when preparing and using disinfectants. When selecting disinfectants for use on items of equipment, check the manufacturer’s guidance before you proceed.
Prepare the correct concentration of disinfectant and allow it to remain on the surface for long enough to achieve effective surface disinfection (see the manufacturer’s recommendations). Concentrations with inadequate dilution during preparation (too high or too low) may reduce their effectiveness. High concentrations increase the risk of exposing people to harmful chemicals and may also damage surfaces.
Note: After cleaning equipment or an area associated with a confirmed or suspected COVID-19 patient, discard solutions and cloths immediately. Although there are some indications for non-touch disinfection methods like spraying and fumigation (fogging), these techniques are not recommended for routine disinfection of indoor spaces due to potential adverse health risks for the user and other people. Refer to Table 1 for indications. Under no circumstances should a person be sprayed with disinfectant.
Selection of disinfectants
Like other coronaviruses, SARS-CoV-2 is very susceptible to disinfectants. Refer to Table 1 for examples of widely used and available disinfectants. Each one has its advantages and side effects; both the scope of application and chemical characteristics of a disinfectant should be considered, alongside local guidelines, before choosing one.
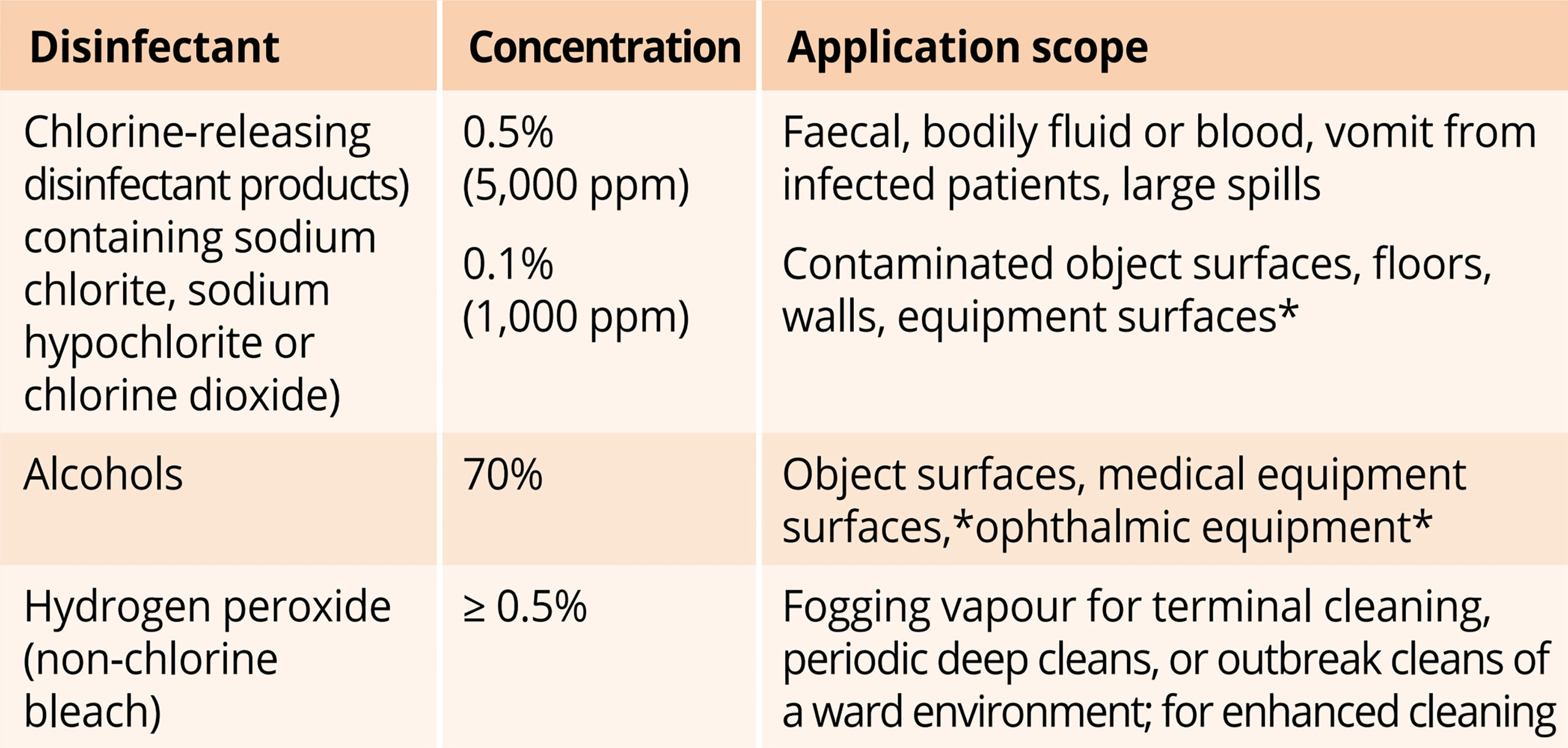
* When a chlorine-containing disinfectant or alcohol is used to disinfect the surface of medical equipment, it is important to consult your medical technicians or manufacturers. Some equipment, in particular metal equipment and electronics, may be sensitive to certain chemicals and they may cause damage. When non-alcoholic disinfectants are applied to surfaces or equipment, wipe down with alcohol or distilled water to remove residues. To prevent electrical shock or damaging electronics, some frequently touched surfaces (such as light switches, phones, computer and keyboards) may be disinfected using 70% alcohol.
How to clean & disinfect: a guide
Cleaning
Clean surfaces thoroughly with a neutral detergent (soap and water). Begin with the cleanest areas first, then move to the more contaminated areas. Clean surfaces that are touched less often before moving on to frequently touched surfaces.
Take care to clean all surfaces, even if they are not visibly dirty. Scrubbing may be necessary to first remove and reduce visible dirt, debris and other organic matter (e.g., blood, secretions and excretions). Organic matter, or ‘soil’, can prevent direct contact of a disinfectant with a surface, so that the disinfectant can’t reach or destroy the microorganisms that may be present.
Clean and disinfect surfaces more often in areas with high traffic, such as outpatient areas and rooms where staff members don and doff PPE.3
Use clean or disposable cloths or paper towels to apply a chemical disinfectant (a chlorine-releasing agent, or 70% ethanol or isopropanol) after cleaning to destroy any remaining microorganisms. Dispose of waste carefully, following standard procedures.
How often?
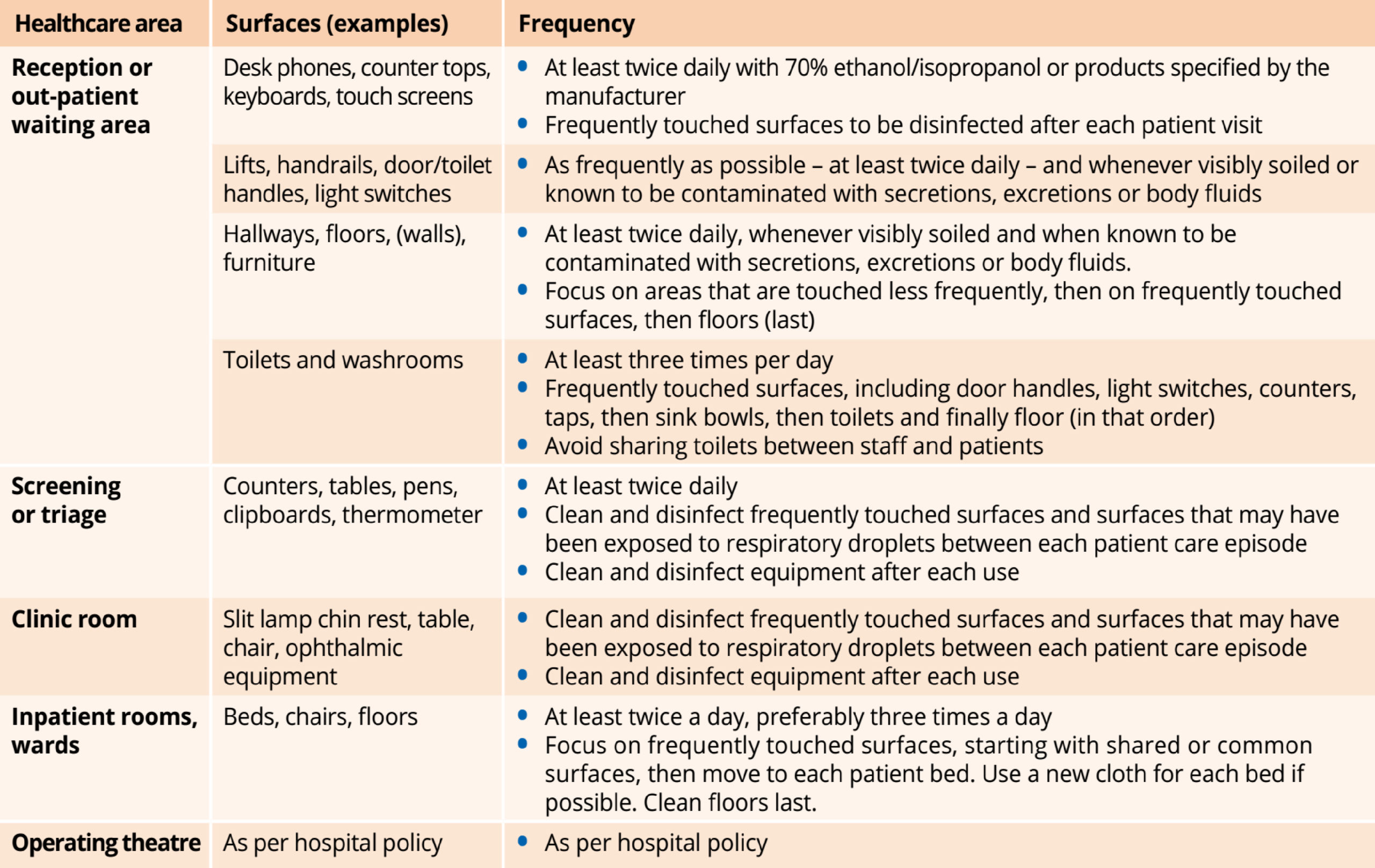
During the COVID-19 pandemic the frequency with which all routine cleaning and disinfection takes place should be increased. Give priority to frequently touched surfaces or contact points such as door handles, for example.4
Selection of disinfectants
Like other coronaviruses, SARS-CoV-2 is very susceptible to disinfectants. Refer to Table 1 for examples of widely used and available disinfectants. Each one has its advantages and side effects; both the scope of application and chemical characteristics of a disinfectant should be considered, alongside local guidelines, before choosing one.
However, it is also important to assess the risk as low, moderate, or high – based not only on the room or area but also on what patient care activities or procedures take place in that space. For example, patient waiting areas are low-risk areas (provided patients are spaced 1–2 metres apart, and there is adequate ventilation), but operating theatres are high-risk areas.
References
1 Kampf G, Todt D, Pfaender S, Steinmann E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J Hosp Infect. 2020 Mar; 104(3):246–251.
2 Damani N. Manual of Infection Prevention and Control 4th ed. Oxford University Press, 2019.
3 Australian Government Department of Health. Health care and cleaning for the health workforce during COVID-19. bit.ly/australiaclean Last accessed 15 July 2020.
4 Public Health England. Reducing the risk of transmission of COVID-19 in the hospital setting. bit.ly/UKclean Last accessed 15 July 2020