Current trends in surgical management of myopia

Related content
Over the last few decades, refractive surgery for treatment of myopia has gained popularity as both a cosmetic procedure to avoid spectacles and as a means of complying with occupational vision standards. Refractive surgery procedures include:
- Incisional refractive surgery
- Excimer laser refractive surgery and
- Intraocular surgery
Incisional refractive surgery
The first report of using an incision to alter the shape of the human cornea was in the 19th century, when Schiotz1 used a limbal relaxing incision in a patient who underwent cataract surgery. In the 1980s Radial Keratotomy (RK) was used to treat thousands of patients with myopia with good predictability; however complications including infection, weakening of the cornea and night vision problems has made RK a more or less obsolete procedure for myopia management.
Excimer laser refractive surgery
This consists of mainly surface ablation techniques and Laser In Situ Keratomileusis (LASIK). Surface ablation includes:
- Photorefractive keratectomy (PRK)
- Laser subepithelial keratectomy (LASEK) and
- Epithelial laser in situ keratomileusis(epi-LASIK).
In PRK, the epithelium is removed either mechanically by scraping it with a blade or chemically by using a diluted solution of ethanol. In the latter approach the epithelial sheet is not repositioned after laser ablation.
In LASEK the epithelial flap is repositioned gently over the ablated tissue.
An alternative surgical procedure to separate the epithelium mechanically by using an epi-keratome was introduced by Pallikaris et al in 2003.2 The technique is widely known as epi-LASIK.
Comparative studies of surface ablation techniques (PRK versus LASEK) have shown similar refractive outcomes. These procedures work best for myopia up to 6D (Dioptres). Laser surface ablation is a better option than epi-LASIK in patients with epithelial irregularities, dry eye syndrome, thin corneas, patients with possible risk of post epi-LASIK flap dislocation and in patients with possible risk of keratectasia.
Laser In Situ Keratomileusis
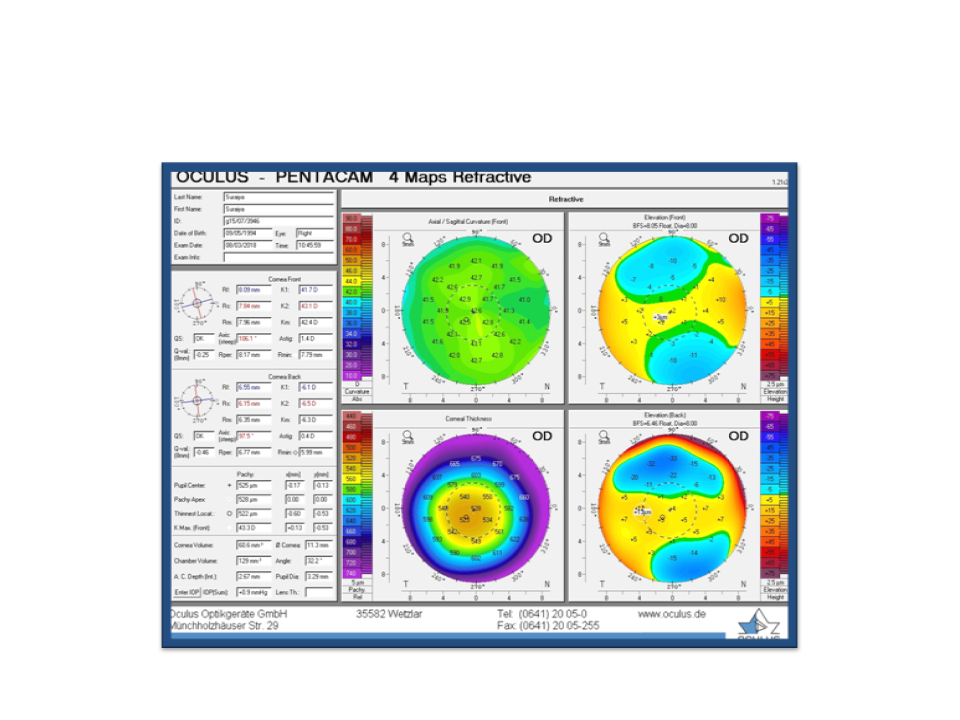
Epi-LASIK is currently the most popular surgical option for myopia correction. It is superior to PRK in terms of patient comfort, visual stabilisations and stromal haze formation. It was first popularised by Pallikaris3 and Buratto4 as a technique of laser ablation of the corneal stroma, which involved the creation of a flap of anterior stroma including Bowman’s and epithelium with the aid of a microkeratome. It can be used to treat up to 15.00D of myopia, however due to risk of long-term ectasia, the recommendation has been revised to a maximum of minus 10.00D (Figure 1).
As with any other surgery, epi-LASIK also has its own share of complications; these include – free flaps, buttonhole flaps, irregular flaps and post epi-LASIK traumatic flap displacement; epithelial ingrowth, dry eye syndrome also need to be kept in mind.
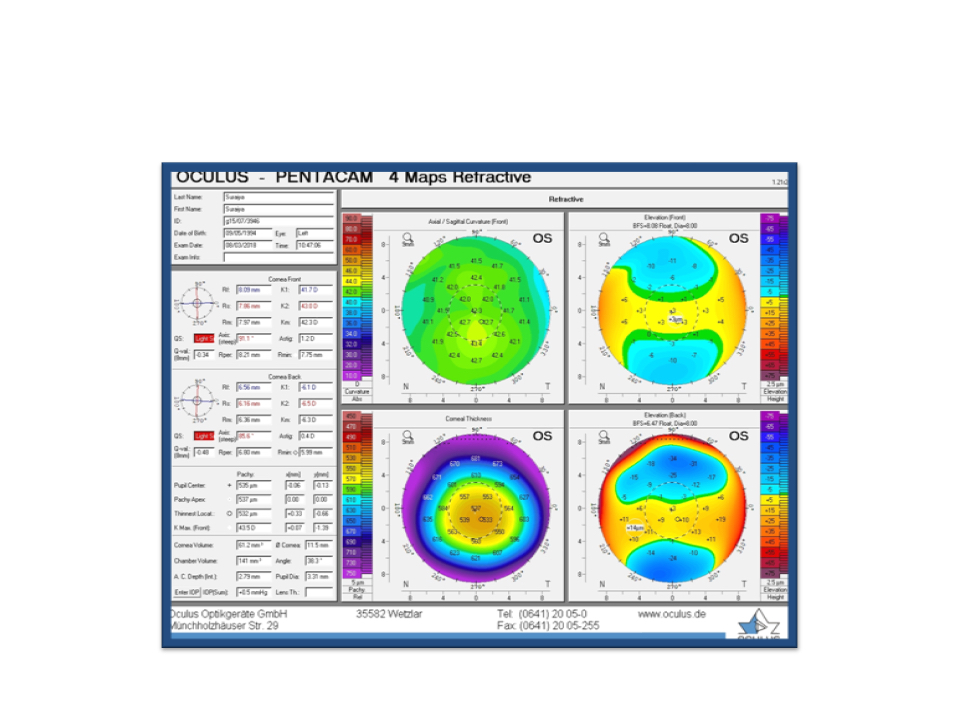
Recently, Wavefront-guided epi-LASIK is being used to preserve the asphericity of the cornea, thus inducing less spherical aberration compared with standard epi-LASIK (Figure 2A and B).
Intraocular surgery
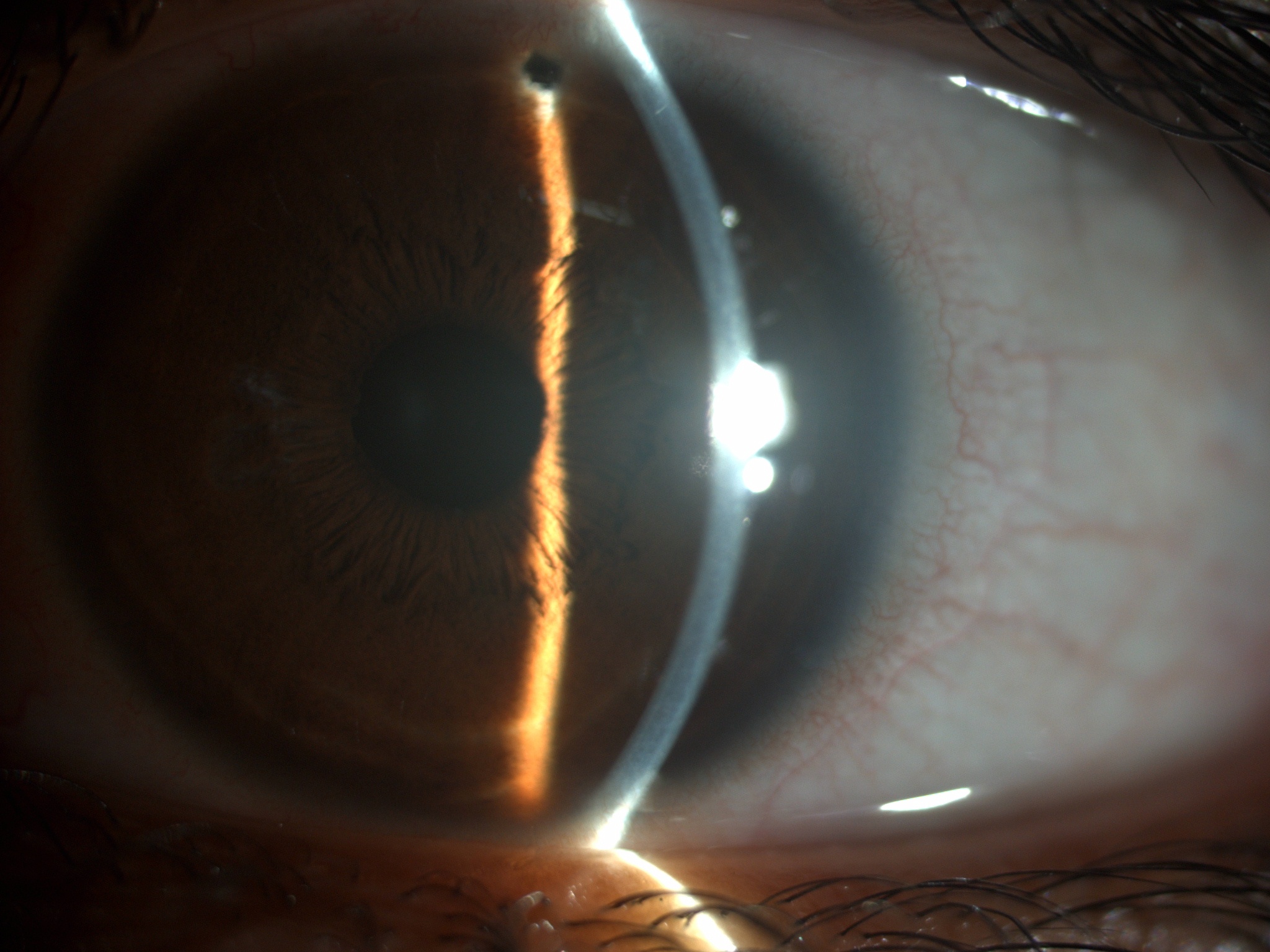
For very high degrees of myopia (more than minus 10D), epi-LASIK is unpredictable and runs a risk of regression and ectasia. Refractive lens exchange (RLE), also known as clear lens extraction, was first described by Fukala in 1890, as one of the options to treat high myopia (Figure 3).5 The availability of a wide range of lens powers both for sphere and cylinder have made this approach more attractive when epi-LASIK is contraindicated. This procedure is best suited for treating high myopia up to myopia -23D, or in other myopes where optical correction or refractive surgery is contraindicated. Even though good refractive outcomes are reported, high myopes run a risk of retinal detachment after surgery, a complication that the patients should be counselled about. Implantation of a Phakic Intraocular Lens (pIOL) can also be considered (Figure 4).

Recent advancements
These days, Femtosecond lasers6 (IntraLase, Irvine, California, USA) have been reported to create more accurate and thinner flaps resulting in more predictable results. The flap dimension can be adjusted based on the needs of patient and the type of excimer laser used. This also aids in faster recovery, and reduces the risk of further corneal problems.
Lastly, the most recent addition to this list is that of SMall Incision Lenticule Extraction (ReLEx® SMILE) which is a minimally invasive procedure, and combines the advantage of both PRK and epi-LASIK – flapless and fast recovery.7 During this procedure, an intrastromal lenticule is created, and is removed from a small 2-3mm tunnel incision. Since 2011, when the procedure started in Europe, China and India, it has proved to be ideal for individuals with active lifestyle/ occupations with a risk of trauma to head or eyes and for those whose are predisposed to chronic dry eye.
Surgical options for refractive errors have come a long way since 1990. In a field like ophthalmology, which is majorly dependent on technology, we only expect the treatment options to become more sophisticated and patient-friendly in the coming years.
References
- Choi DM, Thompson RW, Jr, Price FW, Jr. Incisional refractive surgery, Curr Opin Ophthalmol, 2002; 13:237–41
- O’Keefe M and Kirwan C, Laser epithelial keratomileusis in 2010 – a review, Clin Experiment Ophthalmol, 2010; 38:183–91
- Pallikaris IG, Papatzanaki ME, Stathi EZ, et al., Laser in situ keratomileusis, Lasers Surg Med, 1990; 10:463–8
- Buratto L, Ferrari M, and Genisi C, Myopic keratomileusis with the excimer laser: one-year follow up, Refract Corneal Surg, 1993; 9:12–9
- Packard R, Refractive lens exchange for myopia: a new perspective, Curr Opin Ophthalmol, 2005; 16:53–6
- Binder PS, Flap dimensions created with the IntraLase FS laser, J Cataract Refract Surg, 2004; 30:26–32
- Reinstein DZ, Archer T J, Gobbe M. Small incision lenticule extraction (SMILE) history, fundamentals of a new refractive surgery technique and clinical outcomes. Eye and Vision, 2014; 1:3